This guest blog was written by Fiona McMahon, DPT, and it was posted with permission from Amy Stein, DPT, owner of Beyond Basics Physical Therapy.
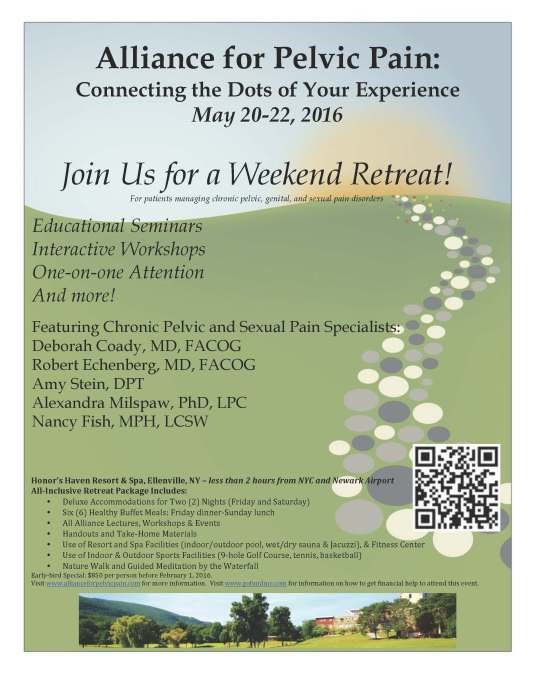
Come participate on May 20-22, 2016 for a patient retreat! Beyond Basics Physical Therapy is partnering with a host of other top experts in the field of Pelvic Pain to hold a weekend long retreat at Honor’s Haven Resort & Spa in Ellenville, NY. This weekend-long retreat is intended for patients (both men and women) who are managing persistent pelvic, genital, back and sexual pain. The retreat will feature educational seminars, workshops, and one-on-one treatment with various healthcare professionals in the field of pelvic pain. Participants will also have the ability to enjoy the many amenities of the resort itself, such as the fitness center, spa facilities, and outdoor/indoor sports facilities.
For patients who need financing for their healthcare journey, consider gofundme.com or request a corporation to sponsor your participation in this wonderful opportunity.
For more information, please check out our flyer or www.allianceforpelvicpain.org and read some of our patient testimonials below. Register early! Spots will fill fast!
“The Alliance for Pelvic Pain retreat was a life-changing experience. It was wonderful to meet so many other women w/ similar symptoms. I felt incredibly supported & understood.”
– 2013 Retreat Participant
“The event was beyond my expectations. I am in my upper twenties and connected to people in all age ranges. I received guidance from older people who also told me how much they respected me for having this challenge at such a young age.” – 2013 Retreat Participant
“I left the conference feeling much more of that sense of integration, and with a sense of connectedness to everyone else there. I have much more I could say about this, but I just wanted to say how deeply meaningful the whole experience was for me and how grateful I am for you to have provided it.” – 2013 Retreat Participant
The Washington Post Article Includes Pelvic Floor Physical Therapy
You know you have successfully convinced your friends about the importance of your profession when not one, but several friends email you the latest major shout out to your profession- an excellent article in the Washington Post about the benefits of pelvic floor physical therapy (link to article). On December 22, 2015, Tara Bahrampour published her article, “The hidden medical epidemic few women have been willing to talk about, until now” which mainly addresses pelvic organ prolapse, descent of the pelvic floor organs. The article also discusses urinary and fecal incontinence.
I’ll recap some of the facts and statistics from the article that I most appreciated:
The age of onset of pelvic floor dysfunction is 56 years old for the average American female
10% of women who experience pelvic floor dysfunction eventually undergo surgical intervention
Pelvic floor muscles tear in approximately 10-15% of vaginal deliveries, thereby interfering with their ability to support the pelvic floor organs
As with many medical related matters, genetics plays a significant role in the development of prolapse, and the condition tends to run in families
Approximately 200,000 of the 320,000 annual pelvic floor corrective surgeries are prolapse related
Invest stock in Depends rather than Always, because more pads are sold for incontinence than for menstruation in the USA. (Even better- tell others about the benefits of pelvic floor physical therapy. No offense to incontinence products, but I look forward to the day when the success of my field will make them obsolete.)
In France, postpartum women are routinely referred for ten sessions of physical therapy after vaginal deliveries
While clearly there were many excellent points raised in the article, I will express my disappointment over one issue. In my humble opinion, pelvic floor physical therapy was only briefly touched upon as an effective intervention. Further elaboration about what to expect during the process and what physical therapists actually teach would have been helpful. There was too much emphasis on pessaries and surgery, and not enough discussion about Kegels, biofeedback, and endurance training. Therefore, I will take the liberty to do so right now. (That comes with the poetic license of writing a blogJ).
Pelvic floor muscle contractions are colloquially referred to as Kegels, and these are the subtle yet powerful exercises that pelvic floor physical therapists teach to appropriate patients who are undergoing a strengthening, or uptraining, program. Biofeedback is a tool utilized by some therapists to help patients create a mind-body connection. Oftentimes, women arrive at physical therapy without prior knowledge of the very existence of their pelvic floor muscles. It is therefore understandable that these women do not know how to properly contract these obscure and small muscles. Biofeedback provides visual cuing to patients, which makes it an especially helpful device when teaching visual learners. A patient is able to see on a computer screen or handheld biofeedback device the amount of electricity being generated by the muscles, represented by a bar or line, at rest, during contractions, and after contractions. Furthermore, the treating therapist can challenge the patient to squeeze the pelvic floor muscles and to hold the contraction for as long as they can. This allows the therapist to assess the patient’s muscle endurance, and it helps them set appropriate endurance goals. Often times, patients experience an “Aha moment” while using the biofeedback (“Oh! That’s what it looks like when I’m contracting the muscles properly? Ok cool, I get it now”), and there is nothing more rewarding for a teacher than watching the integration and understanding of knowledge unfold before their very eyes.
According to Bahrampour, “Pelvic floor physical therapy can help reduce the tension on the ligaments by strengthening the surrounding area, but the service can be hard to find.” If you are reading this blog, then you are one step ahead of the game, for you have already found a clinician who can help you or your loved ones. If you are geographically too far to benefit directly from the amazing services offered at Revitalize Physical Therapy, then it would be our pleasure to help direct you to someone closer who can help. Please contact us with any questions you may have- it is our pleasure to assist you along your healing journey.


 This guest blog was written by Fiona McMahon, DPT, and it was posted with permission from Amy Stein, DPT, owner of Beyond Basics Physical Therapy.
This guest blog was written by Fiona McMahon, DPT, and it was posted with permission from Amy Stein, DPT, owner of Beyond Basics Physical Therapy.