“Sit up straight and mind your posture!” These may not have ever been anyone’s famous last words, but they are definitely ones that most of us have heard at some point or other in our lives. (Would it be terrible were I to confess that I myself was chided on the matter during physical therapy graduate school by one of my very own professors?)
Admittedly, being mindful of one’s posture can be very challenging. It is easy to slack off, slouch off, and fall back into poor habits, pun intended. While old habits die hard, nevertheless practice makes perfect. That being said, I challenge you to commit yourself to improved posture.
On that note, I would like to share some tips for proper standing posture:
- Try to bear your weight on the balls of your feet.
- Keep your knees slightly bent instead of locked in extension.
- Keep your feet approximately shoulder-width apart.
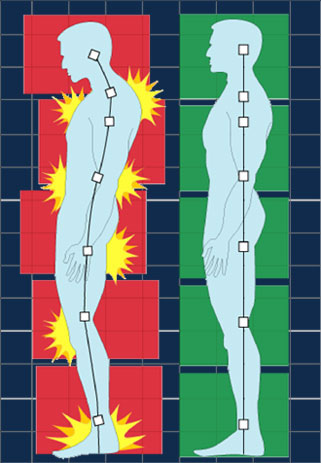
- Stand straight and tall with your shoulders pulled backward. I encourage my clients to keep their ears over their shoulders.
- Try to maintain neutral pelvic position (as in, not rotated too far forward or too far backward). Improved posture contributes to improved musculoskeletal pelvic alignment. This can help reduce symptoms in individuals who experience pelvic pain.
I was recently introduced to an informative video (link to video) created by physical therapy students at Carrington College about proper posture. This short video (approximately 2.5 minutes) provides useful tips about how to adopt improved postural habits. As a person of relatively small stature (i.e. 5’4”…in heels), my favorite part is the usage of a stool to help improve sitting alignment. (Yes, I sat through graduate school with my helpful stool)
Hopefully, this video will help viewers achieve optimal biomechanical alignment.